
Note to first time users: This calculator can be used to calculate tumor response to treatment by the Response Evaluation Criteria In Solid Tumors (RECIST) 1.1., using either the nadir or baseline measurements as reference point. Please go through the detailed ‘Notes’ below if unfamiliar with the RECIST system and criteria for measurements.
Notes
Prerequisites for using RECIST
- CT is the preferred modality for RECIST, though MRI and in some cases even x-ray can also be used.
- The baseline imaging should be done <4 weeks before treatment begins.
- Slice thickness ⩽5 mm and i.v. contrast are required.
Target and non-target lesions on baseline imaging
- On the baseline imaging choose 5 target lesions, which can be reliably measured, and the sum of their longest(!) diameter (SLD) can be calculated
- a maximum of 2 lesions should be in a single organ
- for solid tumors a longest diameter ≥10 mm is the minimum
- for lymph nodes a short axis diameter (SAD) ≥15 mm
- for bone lesions only the soft tissue component can be included in the measurement, entirely sclerotic lesions cannot be used as target lesions.
- In the rare cases where chest x-ray is used for RECIST assessment lung masses ≥20 mm can be used as target lesions.
- Partially cystic or necrotic masses can be used as target lesions, but if possible rather choose solid lesions for this purpose.
- Lesions located in an area which has been subjected to loco-regional therapy (radiotherapy, etc.), are not suitable for target lesions.
- Lesions in mobile organs (e.g. bowels) cannot be reliably compared, and thus are also not suitable.
- Pleural mesothelioma is unique as the tumor thickness perpendicular to the chest wall should be used.
- Non-target lesions can be e.g. malignant pleural effusions or ascites, which are hard to compare numerically, but can be still followed, or inflammatory breast disease, and lymphangitic involvement of skin or lung.
- Any supernumerary lesions which meet the criteria for target lesion should be treated as non-target lesions.
- Solid lesions <10 mm or lymph nodes <15 mm are also considered non-target lesions.
Response categories in the RECIST system
- Complete response (CR)
- disappearance of all target and non-target lesions
- SAD of previously pathological lymph nodes should be <10 mm
- Partial response (PR)
- ≥30% decrease in the SLD of target lesions
- Stable disease (SD)
- neither unequivocal progression or regression
- Progressive disease (PD)
- ≥20% increase in the SLD of target lesions compared to smallest SLD in the study (nadir)
- AND ≥5 mm SLD increase
- OR progression of non-target lesions
- OR new lesions
- lesions in body parts previously not imaged should be considered as new
- bear in mind that e.g. new sclerotic bone lesions during therapy often represent the osteoblastic response of previously undetectable lesions, and are therefore not necessarily new metastases
- PD on the basis of solely non-target lesion progression should be carefully considered. It should be used only if the progression of non-target lesions is sufficiently severe that the behavior of target lesions no longer represents disease burden. Equivocal new lesions should be followed until their behavior can be clearly established.
Evaluating the follow-up examination
- The target lesions have to be measured as long as they are visible, i.e. on follow-up imaging a lymph node with a SAD <10 mm (normal range) must be still measured and included in the SLD.
- If a target lesion disappears use 0 mm as input parameter.
- If a target lesion becomes too small for reliable measurement, but remains visible a 5 mm measurement should be assigned to it.
- If a lesion breaks into two separate smaller lesions then measure the longest diameter of both smaller fragments, and use their sum for calculations.
- If the lesion shows cavitation, it is still the longest diameter that should be measured according to RECIST 1.1. However, it is recommended to indicate in the report that cavitation occurred as this represents a diminished viable tumor volume.
- Lesions that disappeared at nadir, then reappear can pose a challenge if the lesions are very small. E.g. in a case where all solid target lesions disappeared at nadir, then at the current examination there appears to be a re-emerging 4 mm lesion due to the rule of ≥5 mm SLD increase PD can not be declared. The calculator will not provide a recommendation in this rare case.
- The SAD of target lymph nodes has to measured and included in the SLD even if it decreased into normal range (<10 mm). This can have profound implications if most or all target lesions are nodal lesions and there had been CR at the nadir. E.g. we are following two nodal metastases (SAD at nadir 8 mm for both, thus CR). The SAD of these lymph nodes have now increased to 10 and 11 mm respectively, putting them in the pathological range again. Also, an about 30% growth and 5 mm absolute SLD change occurred, indicating PD. In these situations ultimately small differences in measurements can result in dramatic change of response category, thus caution is particularly warranted.
Oligoprogression
Oligoprogression is an emerging concept in oncology, indicating a state where most metastases show partial/complete response, while a single or few metastatic foci progress. Oligoprogression is caused by the emergence of novel tumor cell phenotypes during the divergent clonal evolution of the metastatic lesion. It is not formally incorporated into the RECIST 1.1 system. It is worth indicating on the report however if an oligprogressive pattern is suspected. I have written a short summary article about this for Radiopaedia.org a bit earlier.
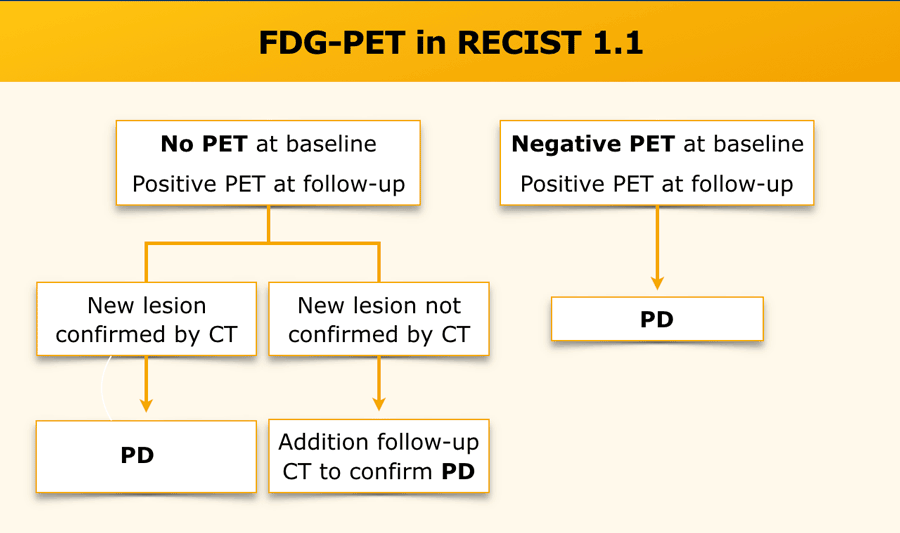
FDG-PET and RECIST 1.1
- A positive FDG-PET during follow-up represents progression IF there was a negative baseline PET-CT. If there was no negative baseline PET-CT then progression should be confirmed by the contrast enhanced CT exam
- This flowchart by Radiology Assistant summarizes the diagnostic algorithm in this case
{kind=link}
Further reading
- Two excellent summary articles of the RECIST 1.1 system with numerous illustrations can be found on the Radiology Assistant here and here. Some imaging examples of the various RECIST categories have been also provided.
- Radiopaedia.org also has a succinct summary article, and a comparison of RECIST 1.1 and the earlier 1.0 system
- This comprehensive review article (open access) provides an excellent overview of the RECIST system:
Last updated: 2021-11-05